The patient is a 76-year-old female who presents with spots on the axilla and flank that have been present for about a year, if not more. The patient does have a history of hyperthyroidism and osteopenia, as well as hypertension. Clinical examination disposes clustered white papules on the bilateral flank and axilla. The clinical differential diagnosis encompasses papillary dermal elastolysis with pseudoxanthoma elasticum light changes clinically, other forms of anetoderma and fibroelastolytic papulosis.
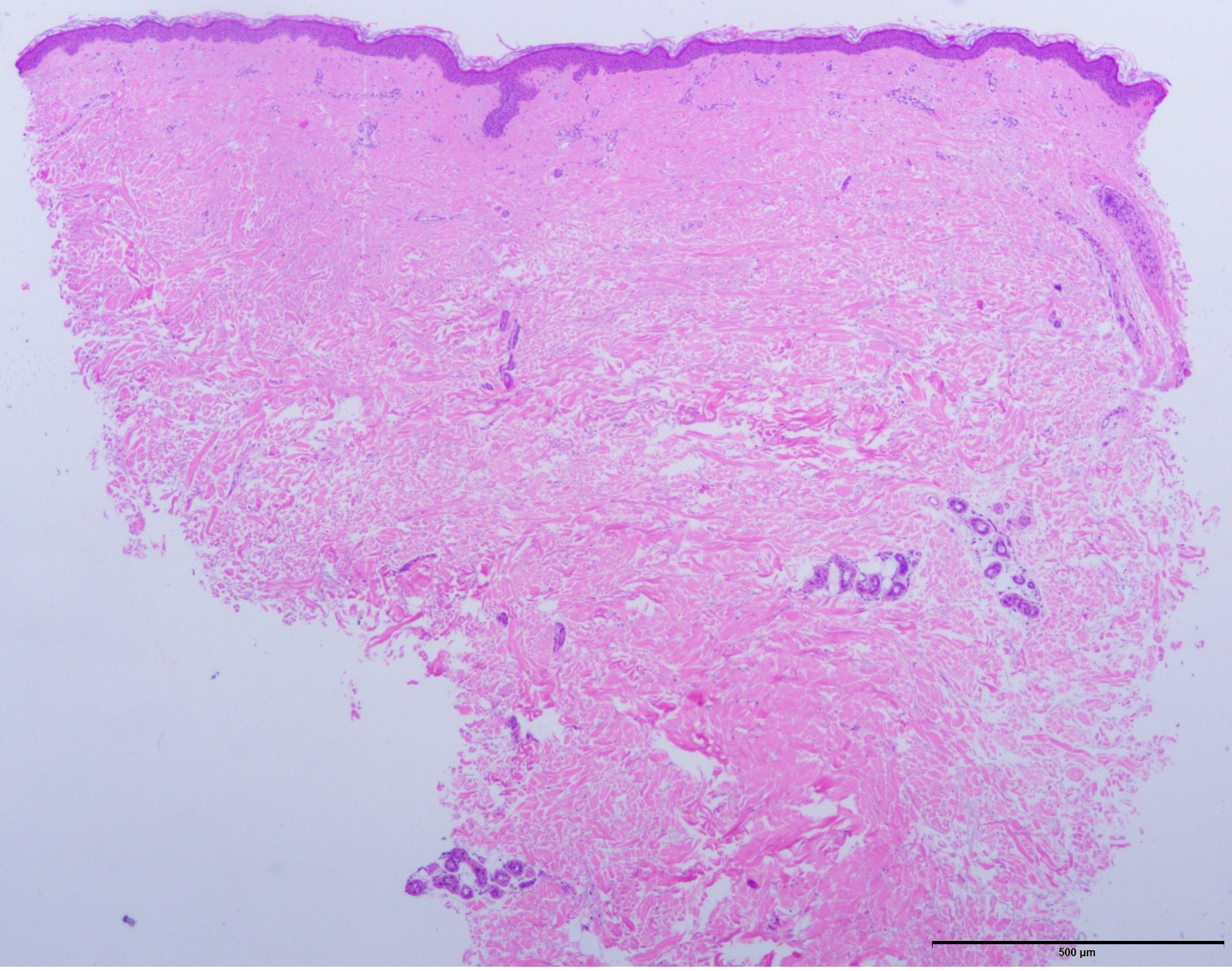
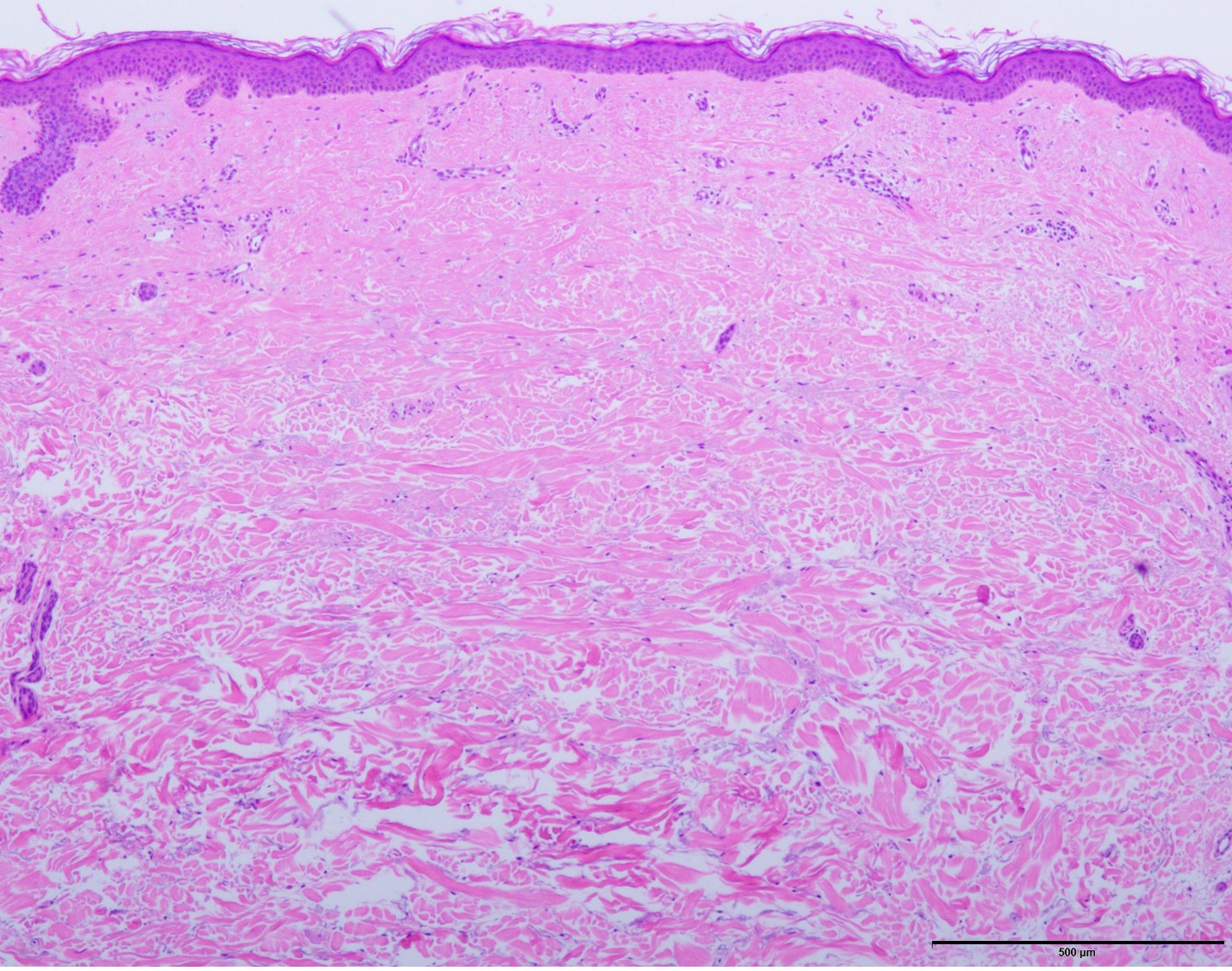
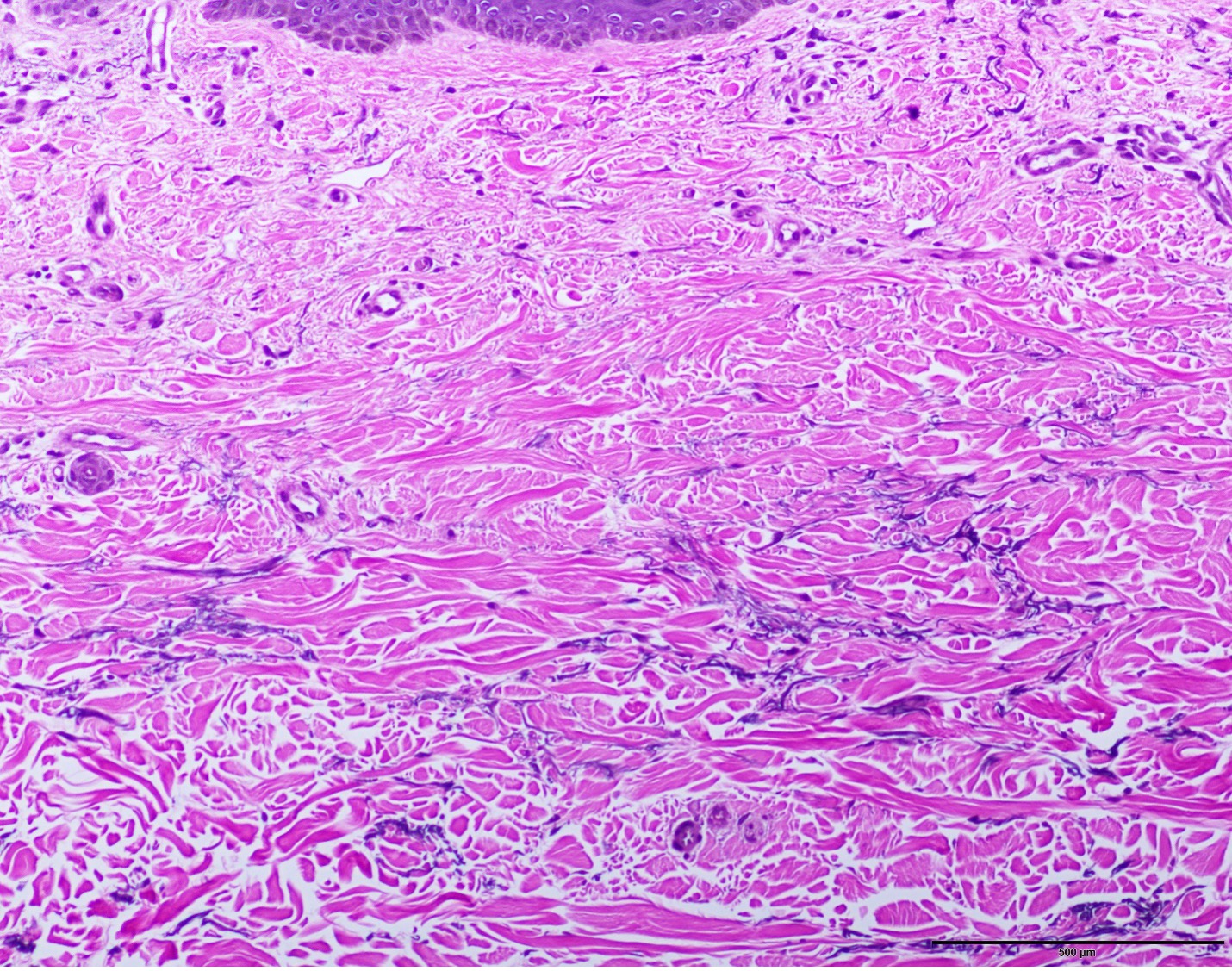
The biopsy does show an anetodermic process characterized by a discrete area of elastolysis within the superficial to mid reticular dermis. The overall morphology is most consistent with a unique form of anetoderma, namely mid-dermal elastolysis which has a very strong association with autoimmune thyroid disease. Indeed, this patient does have a history of hyperthyroidism. Mid-dermal elastolysis is a female-centric disease whereby there are three morphological subtypes of mid-dermal elastolysis. One is characterized by the distinct wrinkling of the skin that follows the cleavage lines, a representation this is not evident in this patient. The second variant is in the context of miniature soft papular lesions, some of which are folliculocentric. Finally some patients exhibit reticular erythema.
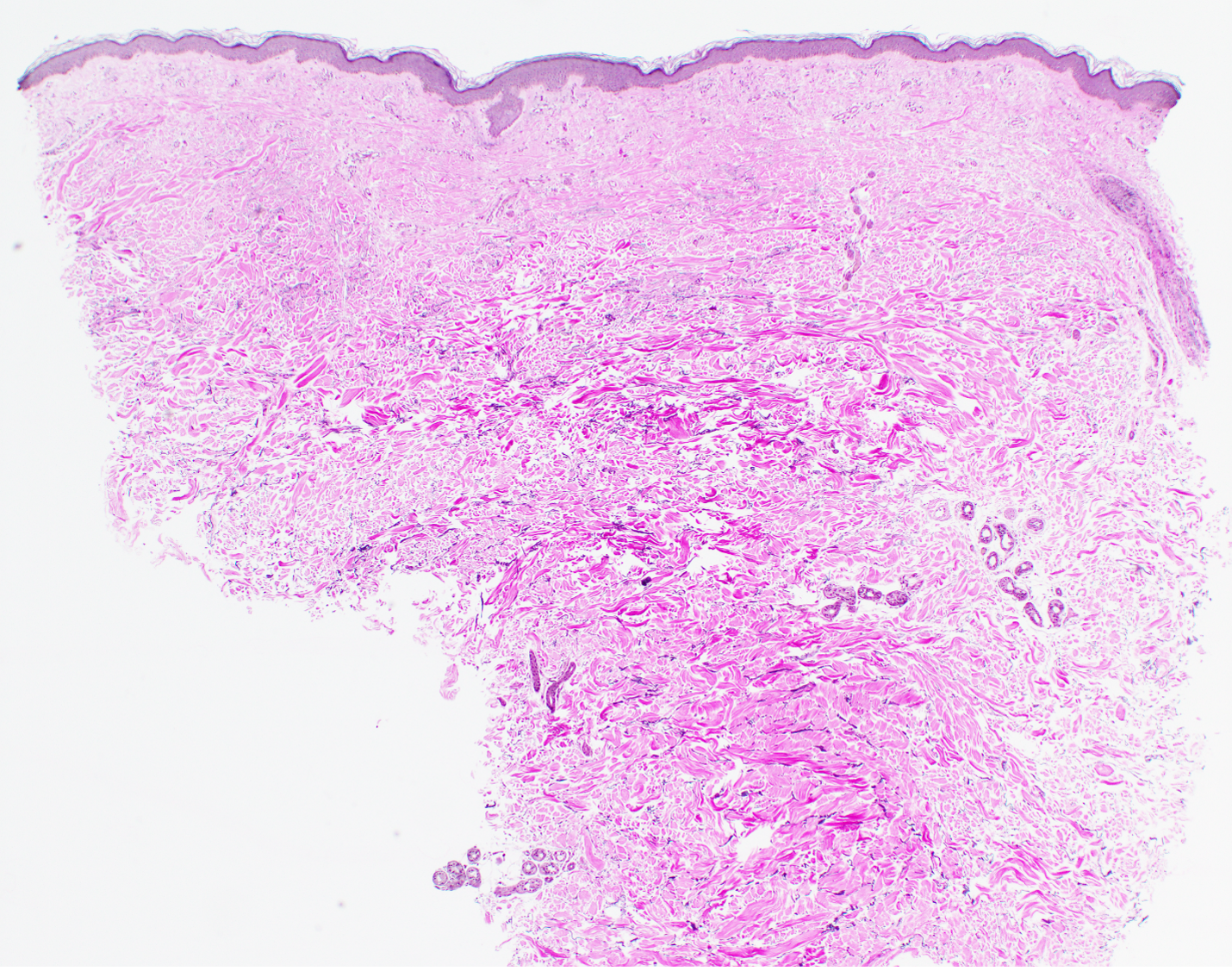
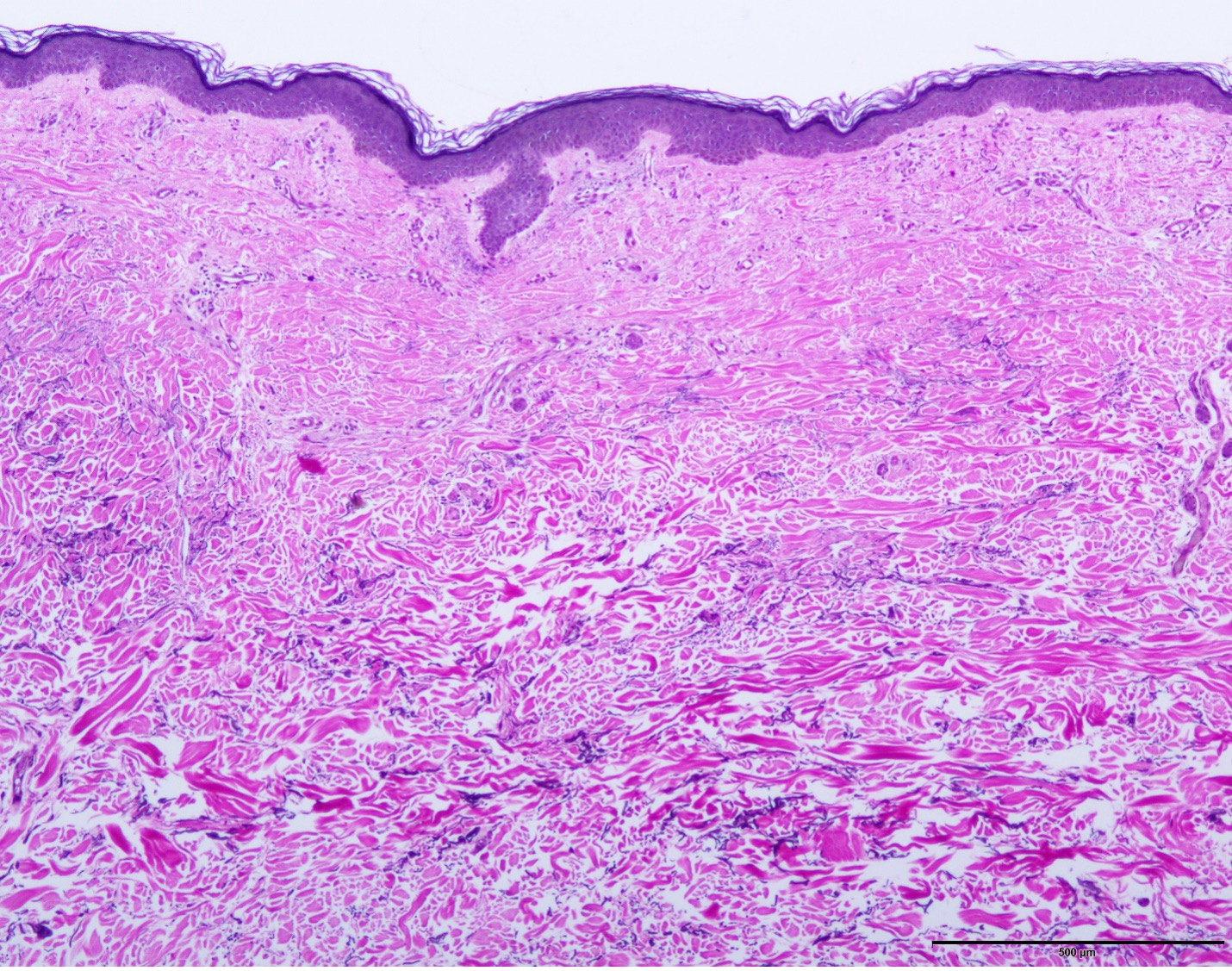
When one examines the photomicrograph of mid-dermal elastolysis, the histology is quite similar to this case. While designated as mid dermal elastolysis in point of fact it is the superficial reticular dermis where the discrete zone of elastolysis is most apparent.
The main sites of involvement include the trunk, shoulders, back, and upper extremities with sparing of the palms, soles, and face.
An inflammatory phase may presage the elastolysis. Some cases may be exacerbated by sun exposure. Over and above thyroid disease other disease associations include rheumatoid arthritis and antiphospholipid antibody syndrome.
While this particular biopsy is pauci-inflammatory, there can be an earlier inflammatory phase that in fact resembles annular elastolytic granuloma. Its etiologic basis is somehow linked with an enhancement of matrix metalloproteinase production. There are certain endogenous inhibitors, likely alpha macroglobulins and other tissue inhibitors of metalloproteinases. Estrogen may prove to be valuable in controlling metalloproteinase activity. Novel therapies designed to downregulate metalloproteinase expression might be considered.
Click images to begin the slideshow