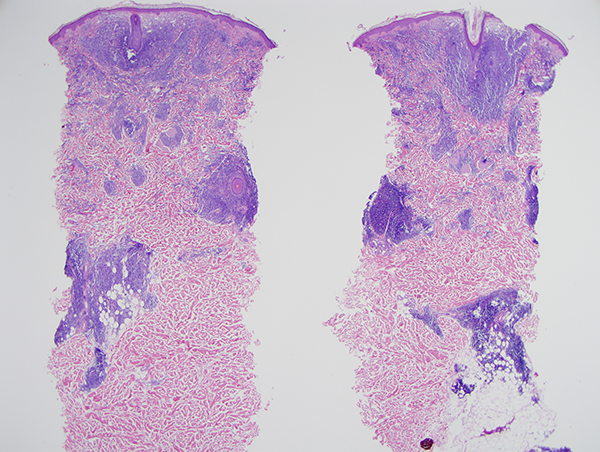
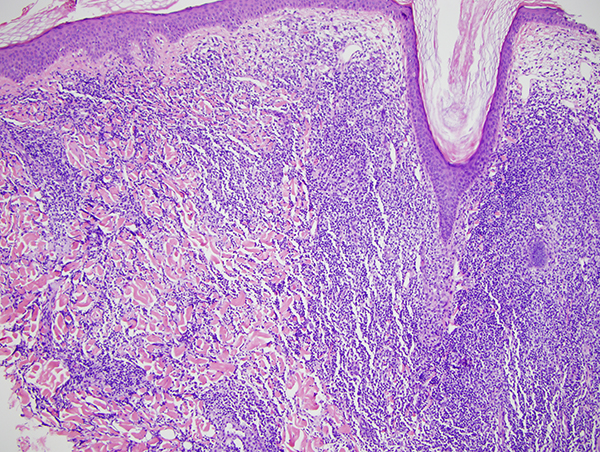
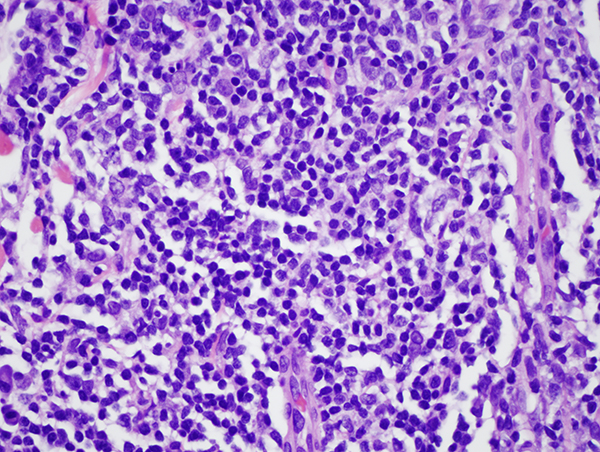
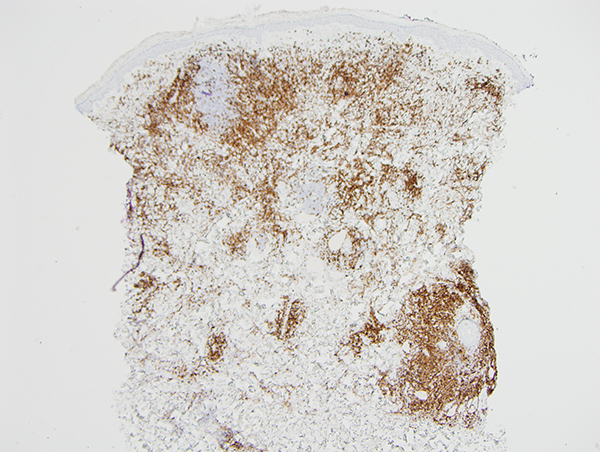
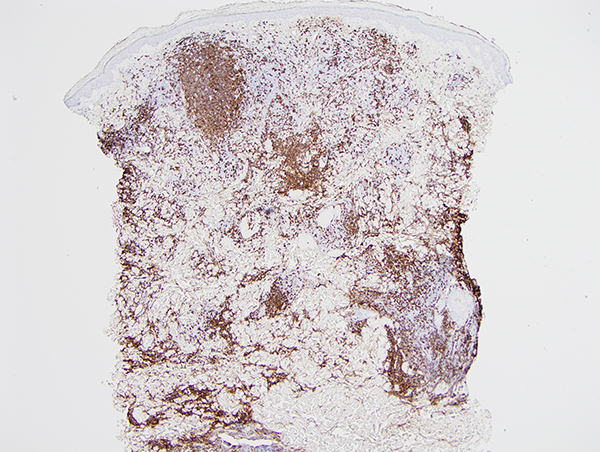
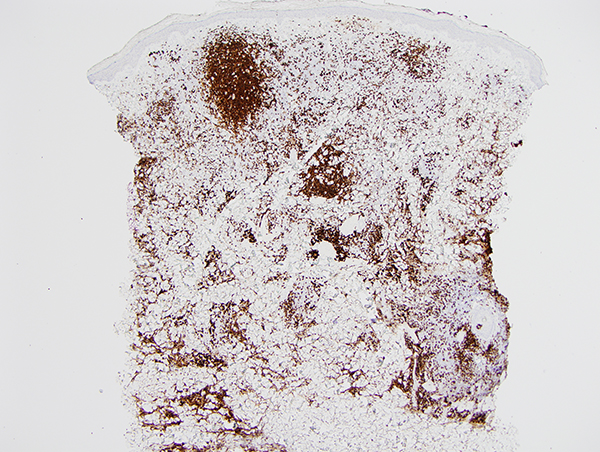
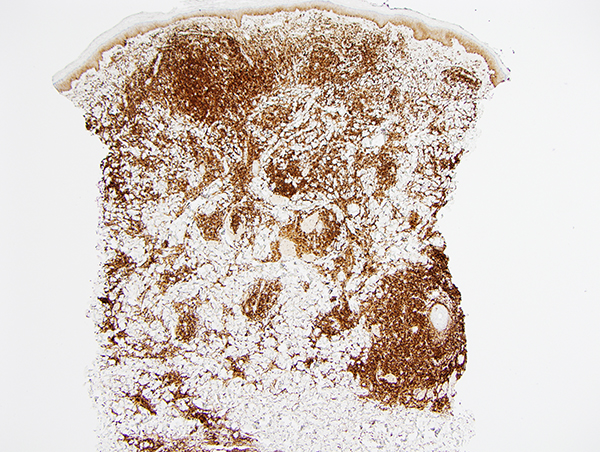
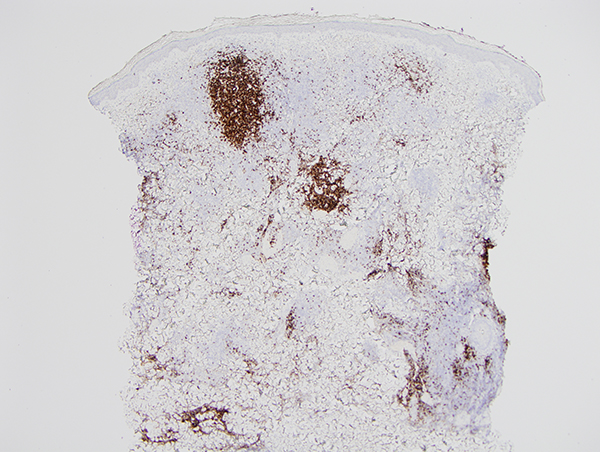
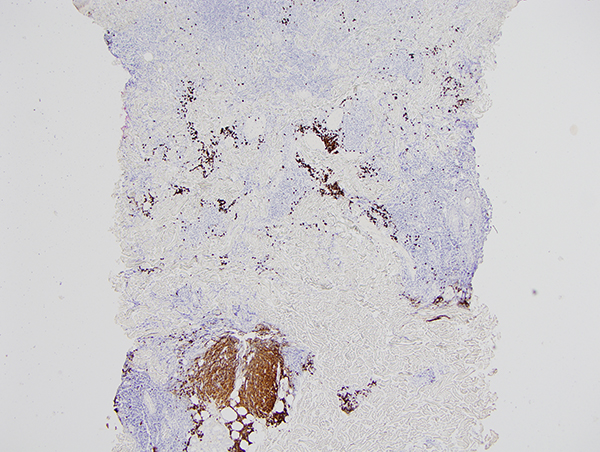
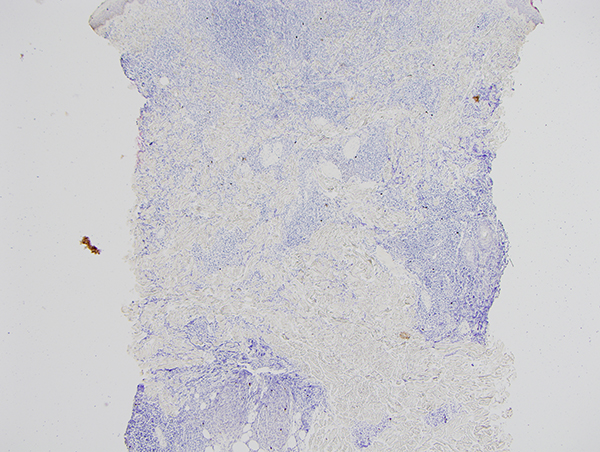
The findings are diagnostic of a well differentiated kappa light chain restricted marginal zone lymphoma; the small nonplasmacytic neoplastic B cells are CD23 positive. There is no evidence of blastic large cell transformation nor of epidermotropism. There is a background of significant benign reactive T cell lymphoid hyperplasia. This type of T cell enriched plasmacytic marginal zone lymphoma characteristically has a very indolent clinical course without extracutaneous disease as opposed to the B cell dominant form of marginal zone lymphoma exhibiting a minimal degree of T cell infiltration. In T cell rich marginal zone lymphoma the neoplastic plasma cells are oftentimes class switched and the infiltrate exhibits a multinodular growth pattern accompanied by many mast cells and regulatory T cells. In the B cell dominant variants of marginal zone lymphoma the B cells are CXCR3 positive without class switching and a greater propensity for extracutaneous disease. In younger patients, there may be a role for iatrogenic immune dysregulation in the propagation of marginal zone lymphoma most notably in regards to chronic antidepressant and antihistamine therapy. In these drug associated cases, the marginal zone lymphoma arises from a background of reactive lymphoid hyperplasia.
Click images to begin the slideshow