- The patient is a 36-year-old healthy female that developed linear depression of her right forearm as of November 2020. A biopsy was performed to rule out linear scleroderma versus eosinophilic fasciitis due to the clinical laboratory finding of a positive antinuclear antibody. Other clinical stigmata of autoimmune disease are not present.
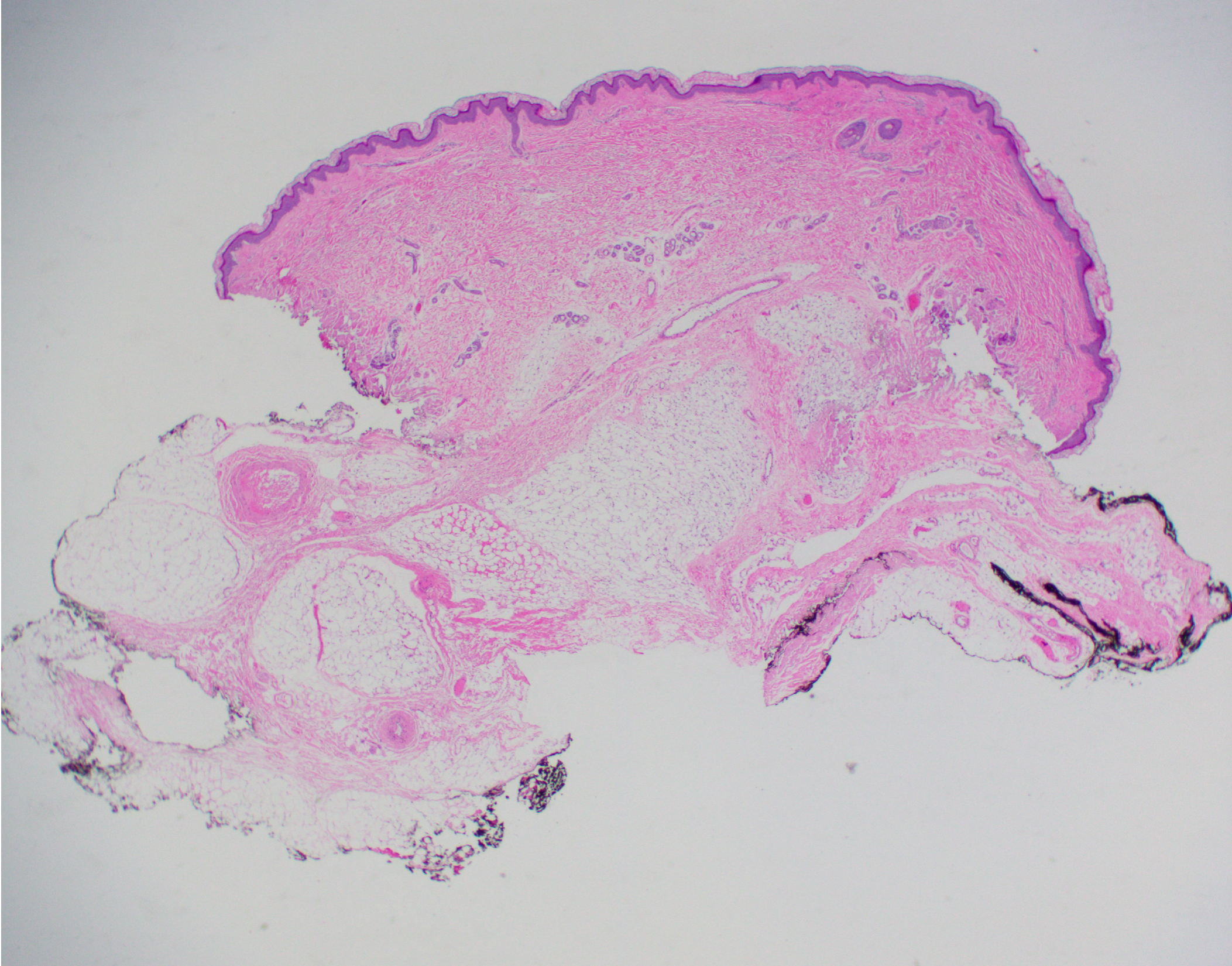
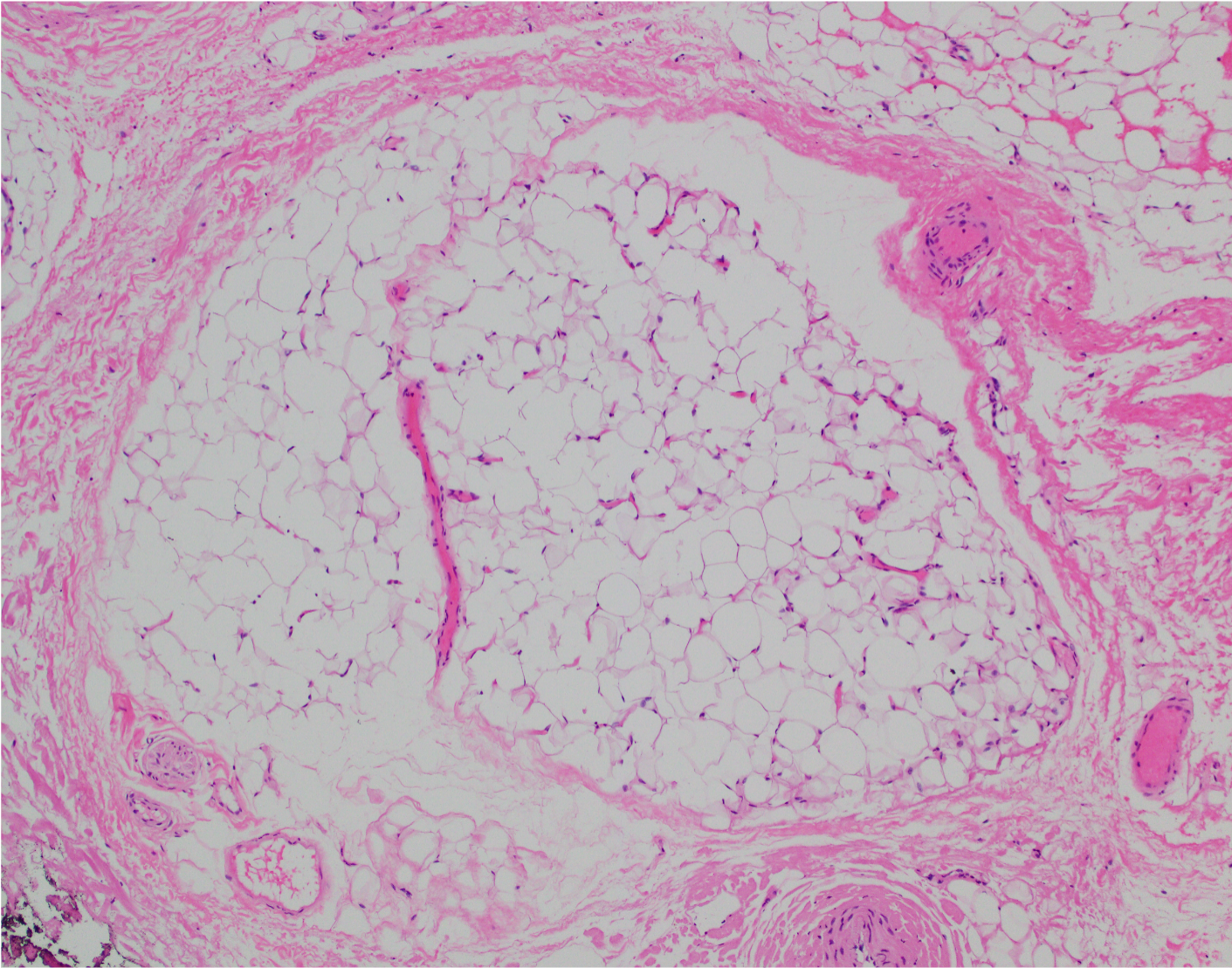
- The biopsy findings do not show any histologic features of an autoimmune sclerodermoid reaction, nor is there is any type of inflammatory process such as lupus erythematosus including lupus profundus including a sclerodermic variant of lupus profundus. The main abnormality is significant lipoatrophy.
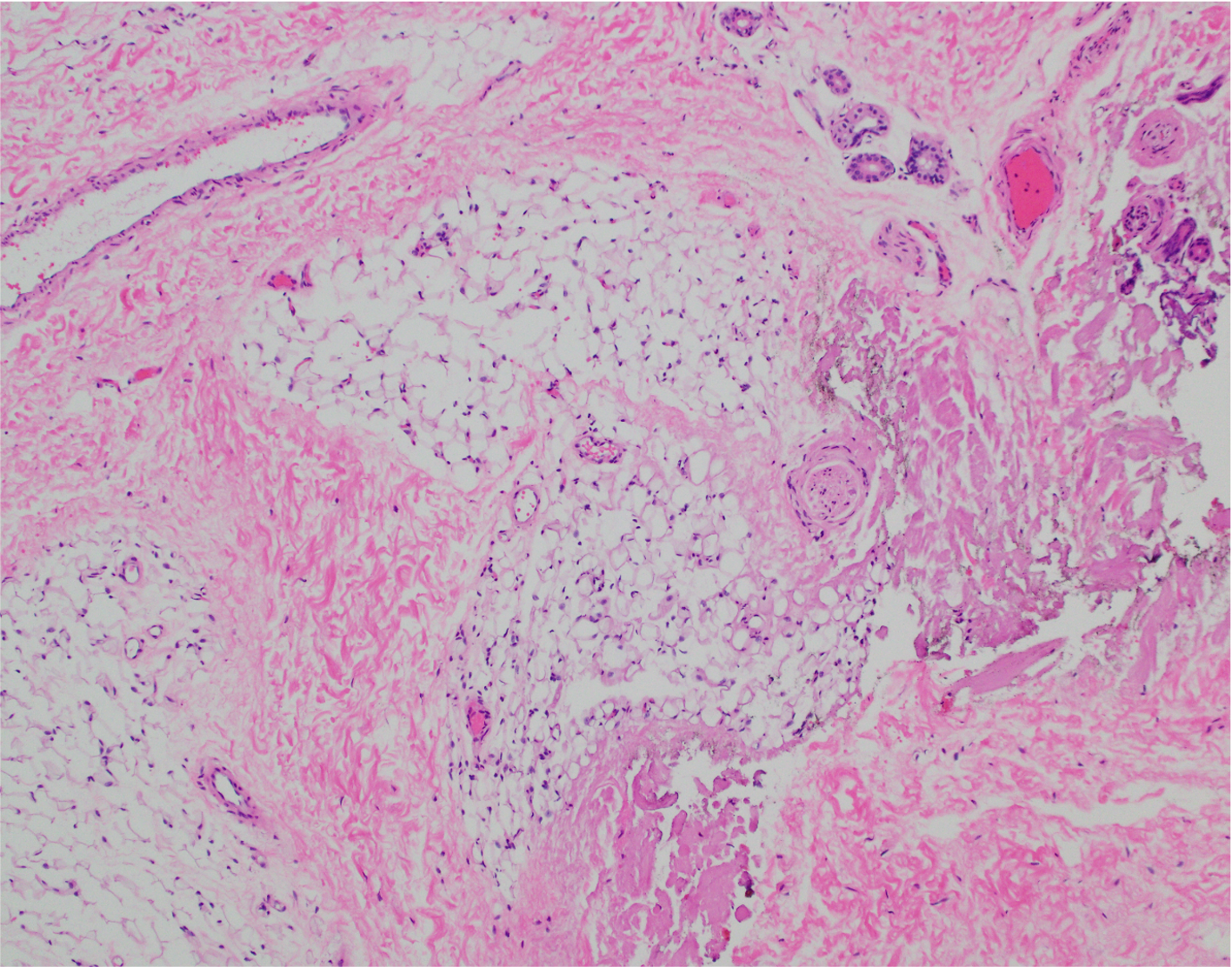
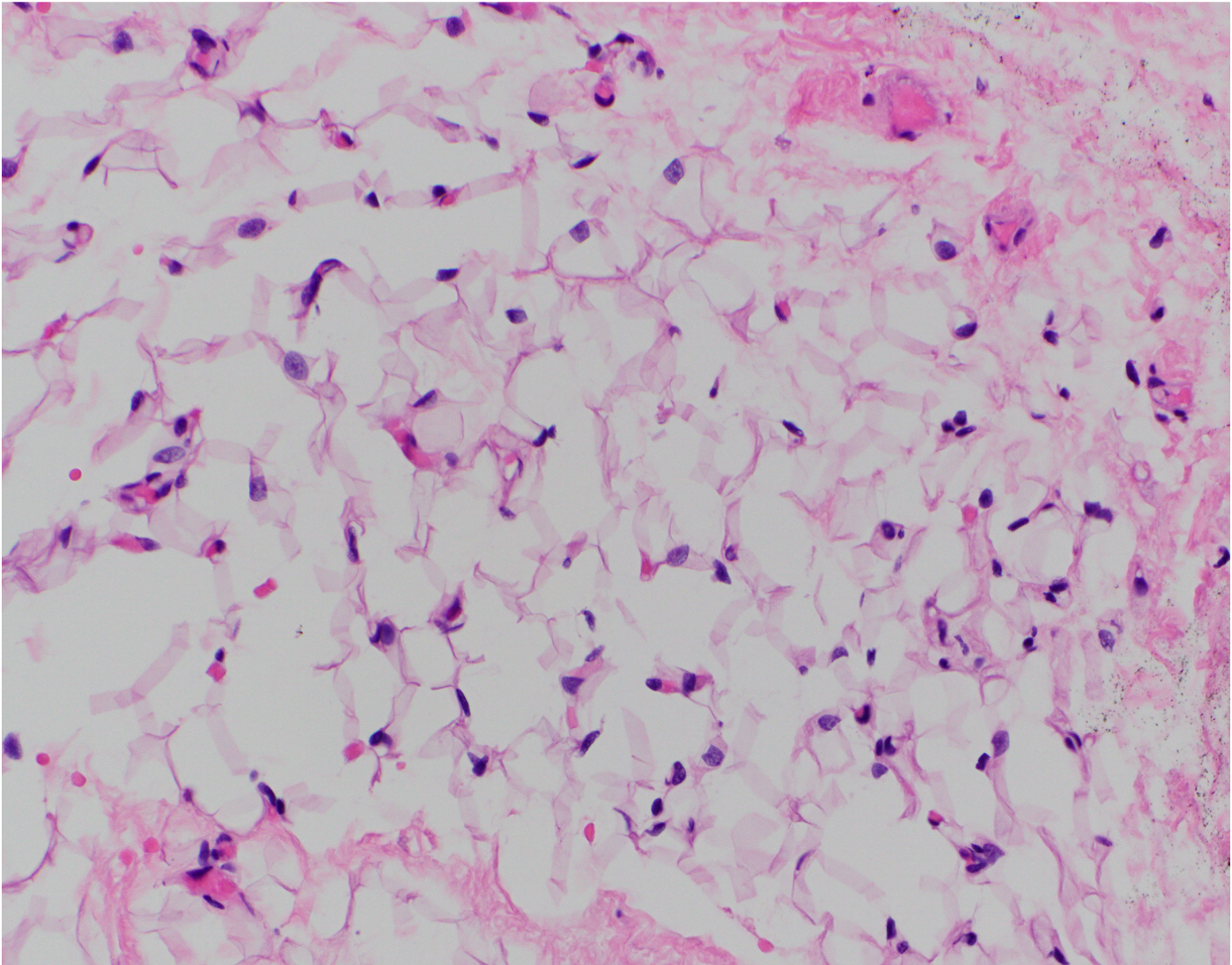
- While lipoatrophy may occur subsequent to a highly inflammatory process in the fat such as lipoatrophic panniculitis, lupus profundus or morphea hence defining secondary lipoatrophy, in this case there is neither inflammation nor fibroplasia.
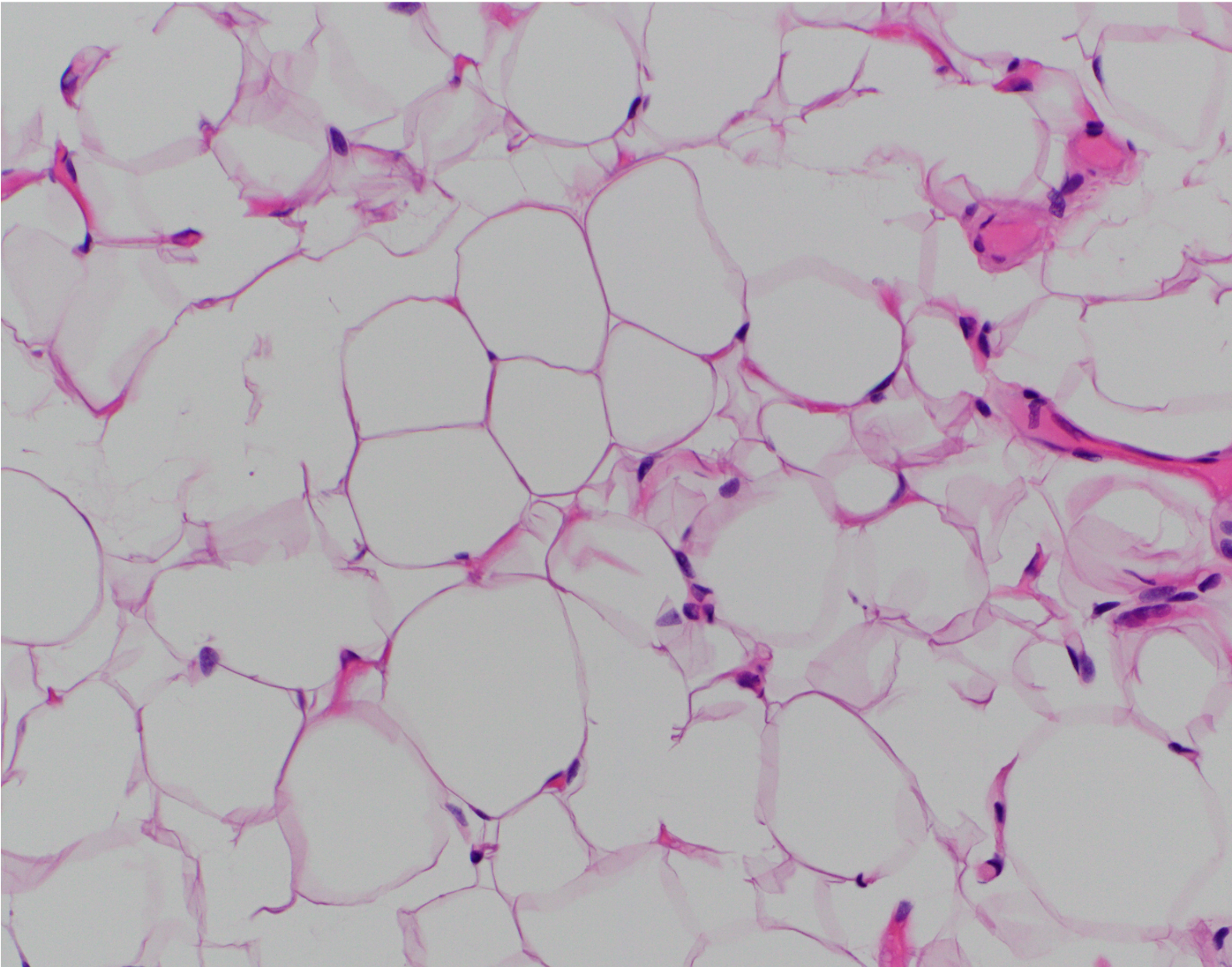
- The classic cause of pauci-inflammatory linear lipoatrophy mimicking linear scleroderma clinically is one of acquired linear lipoatrophy following intraarticular triamcinolone injection into the joint. The patient had intraarticular steroid injections into the wrist, whereby shortly following the steroid injections, the patient began to develop a linear depression which may have continued to progress following an additional intraarticular steroid injection in 2021.
- There is limited literature precedent on this complication, but it does exist. The exact basis of steroid-induced linear lipoatrophy is not fully understood, but crystallization of the steroids into venous and lymphatic channels proximal to the injection leading to localized lipolysis is a consideration. Triamcinolone is poorly soluble in water, so crystals could persist for months within the vasculature. Many of these cases can spontaneously resolve six to twelve months following the corticosteroid injection.
Click images to begin the slideshow