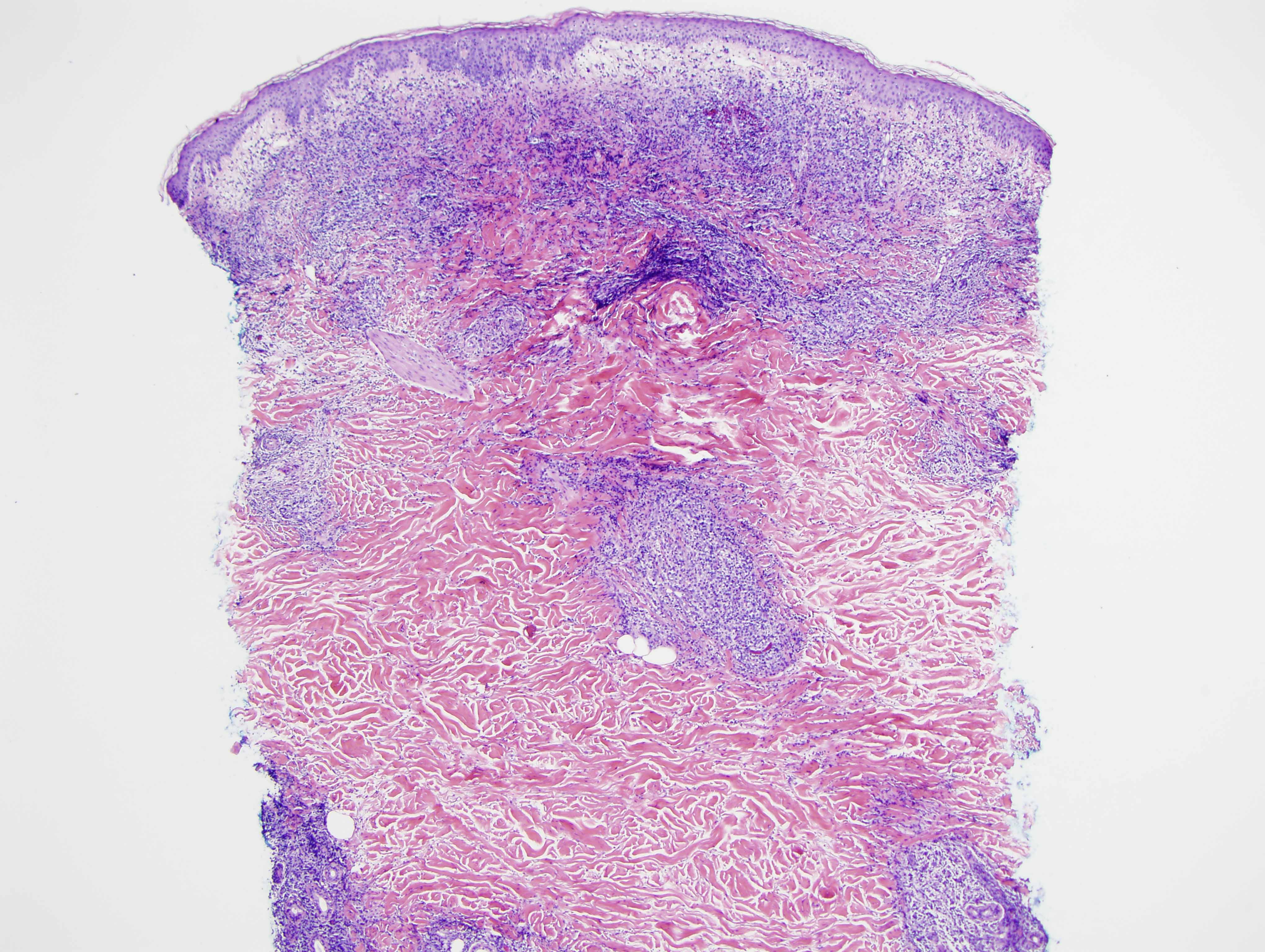
The patient is an 89 y/o male who presented with an explosive onset of a generalized skin rash that clinically resembled pityriasis rosea. The rash differs from classic pityriasis rosea as a number of the lesions were fairly infiltrative plaques and as well there was a plum-colored nodule in the wrist area. The patient otherwise feels well.
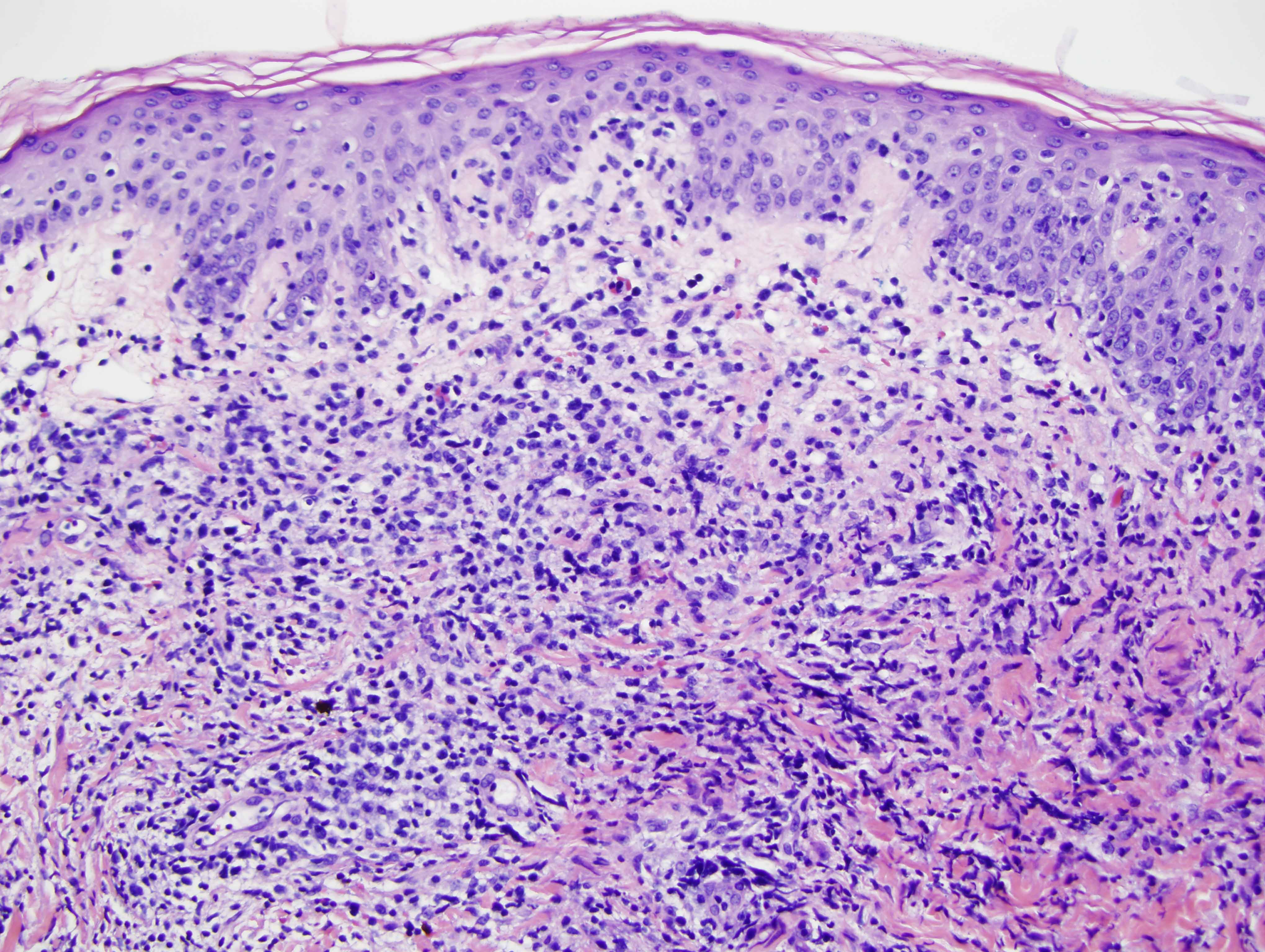
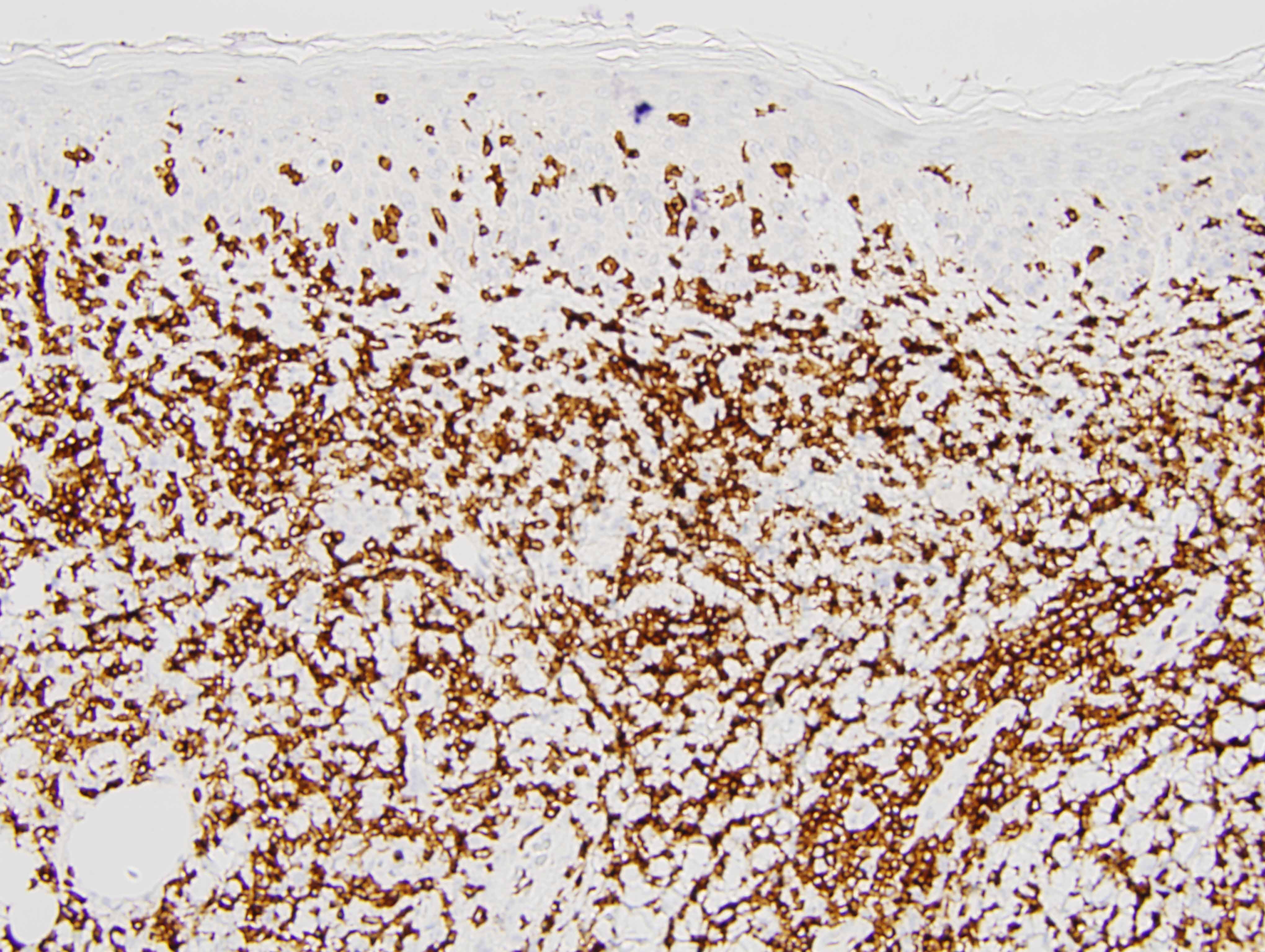
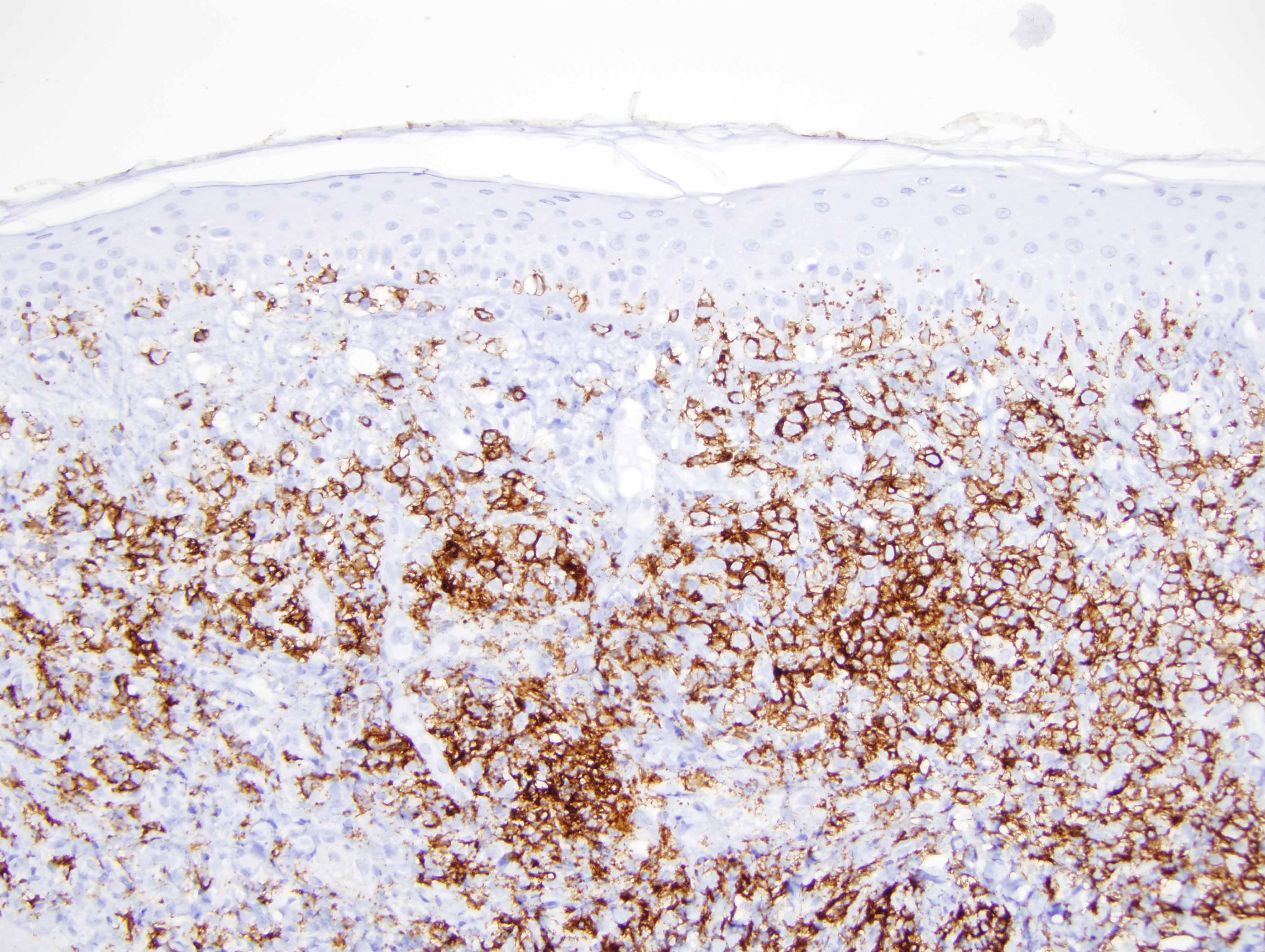
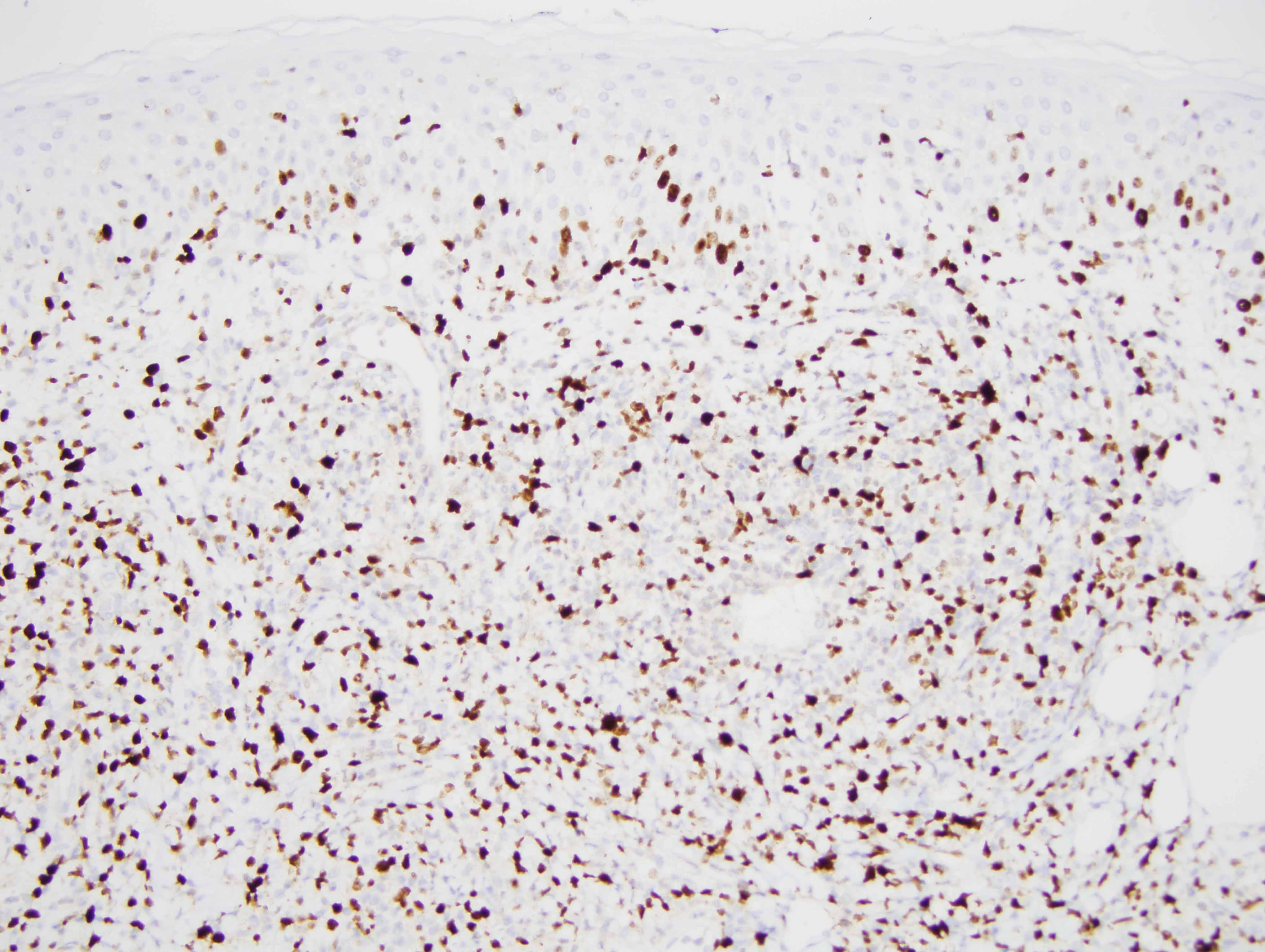
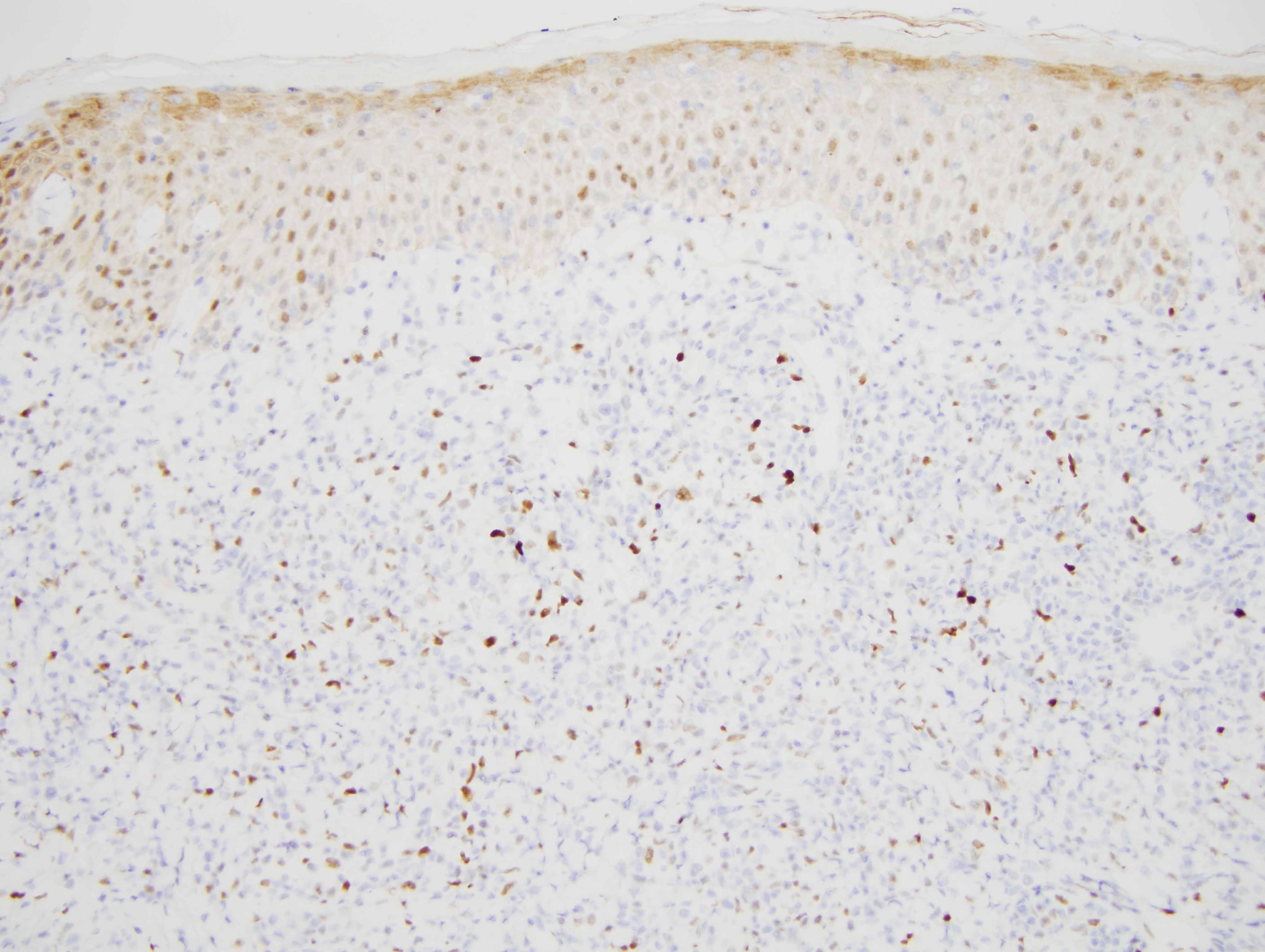
This distinctive clinical presentation along with the histomorphology and phenotypic profile is diagnostic of a very rare form of B-cell lymphoma consistent with so-called epidermotropic B cell lymphoma. In fact the epidermotropic properties are present on all three biopsies but are best exemplified by the original biopsy where an interesting pattern of neoplastic B-cells colonizing the basal layer of the epidermis is observed. As with other cases of epidermotropic B-cell lymphoma the cell of origin does not appear to be of follicle center derivation based on the lack of staining for CD10 and BCL6 on our repeat stain. The neoplastic B cells express an activated phenotype in that they are bcl-2 and MUM-1 positive and also express IgG. It has been postulated that this form of B-cell lymphoma is of marginal zone derivation and indeed the phenotypic profile would be consistent with this construction
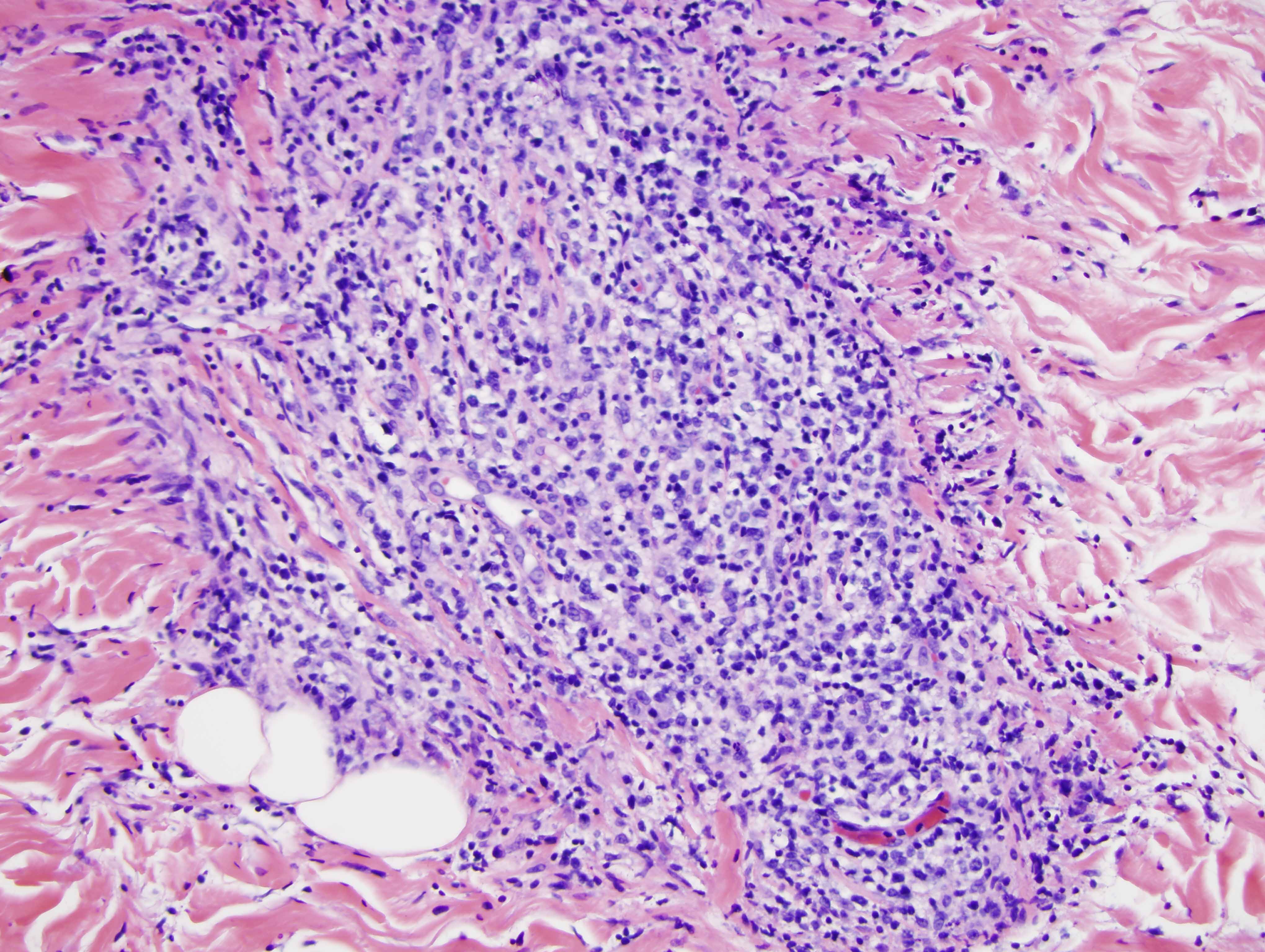
Large cell transformation is a feature of this particular case. We have encountered large cell transformation in the past in epidermotropic marginal zone lymphoma. A very unique feature of this case is the angioinvasive and perineural invasion in a fashion somewhat reminiscent of the type of angiotropic B-cell lymphomas that occur in the setting of lymphomatoid granulomatosis.
The concept of epidermotropic B cell lymphoma as a distinct form of B-cell neoplasia is an emerging one. There is almost exclusive involvement in older men presenting with a distinctive pityriasis rosea-like rash. These patients are often times otherwise asymptomatic although investigations frequently do disclose splenic involvement as well as bone marrow involvement. The clinical course is one that does respond very well to chemotherapeutic intervention with an overall excellent prognosis despite clinical and h stomorphologic features that could be indicative of a more aggressive clinical course (i.e., the degree of angioinvasion and large cell transformation).
Click images to begin the slideshow